Carpal Tunnel Syndrome: Understanding Wrist Pain and Nerve Decompression
- Colin Hurd
- 20 November 2025
- 15 Comments
Wrist pain that keeps you up at night? Tingling in your thumb, index, or middle finger that feels like a phone buzzing under your skin? If this sounds familiar, you might be dealing with carpal tunnel syndrome - one of the most common nerve problems in adults. It’s not just a "repetitive strain injury" from typing too much. It’s a real, measurable compression of the median nerve as it squeezes through a tight tunnel in your wrist. And if left untreated, it can lead to permanent weakness and loss of function.
What Exactly Is Carpal Tunnel Syndrome?
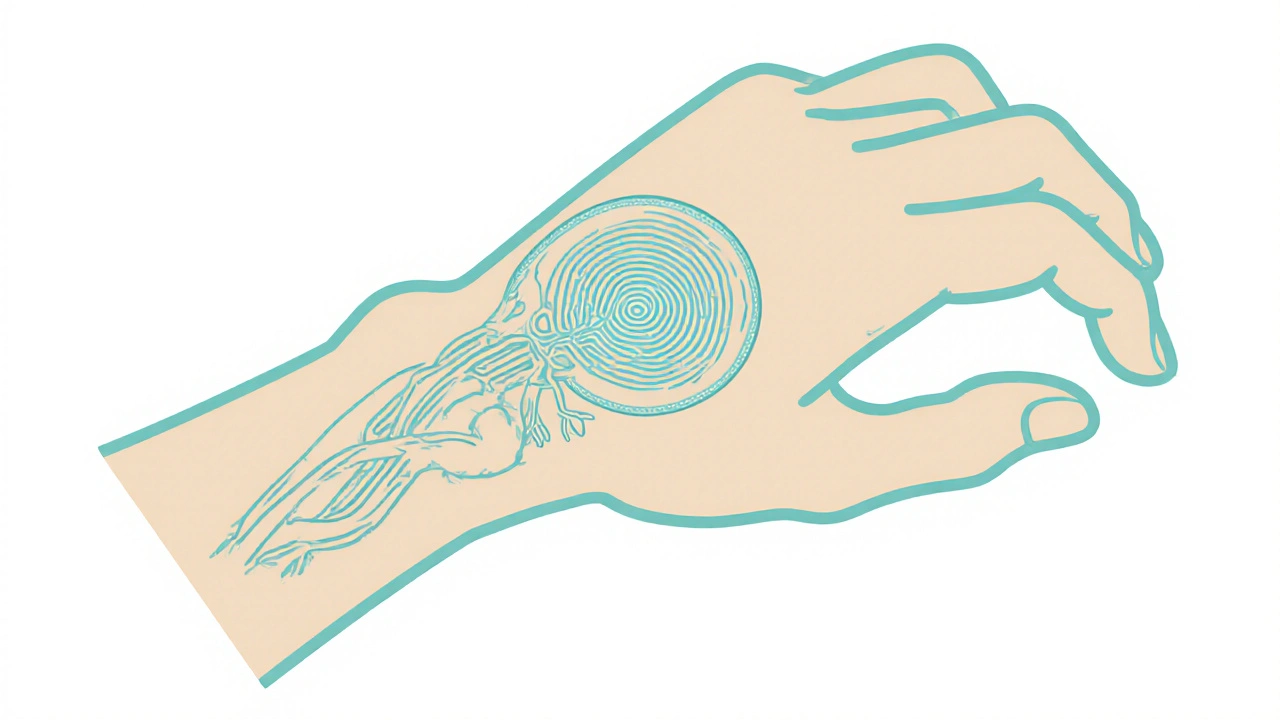
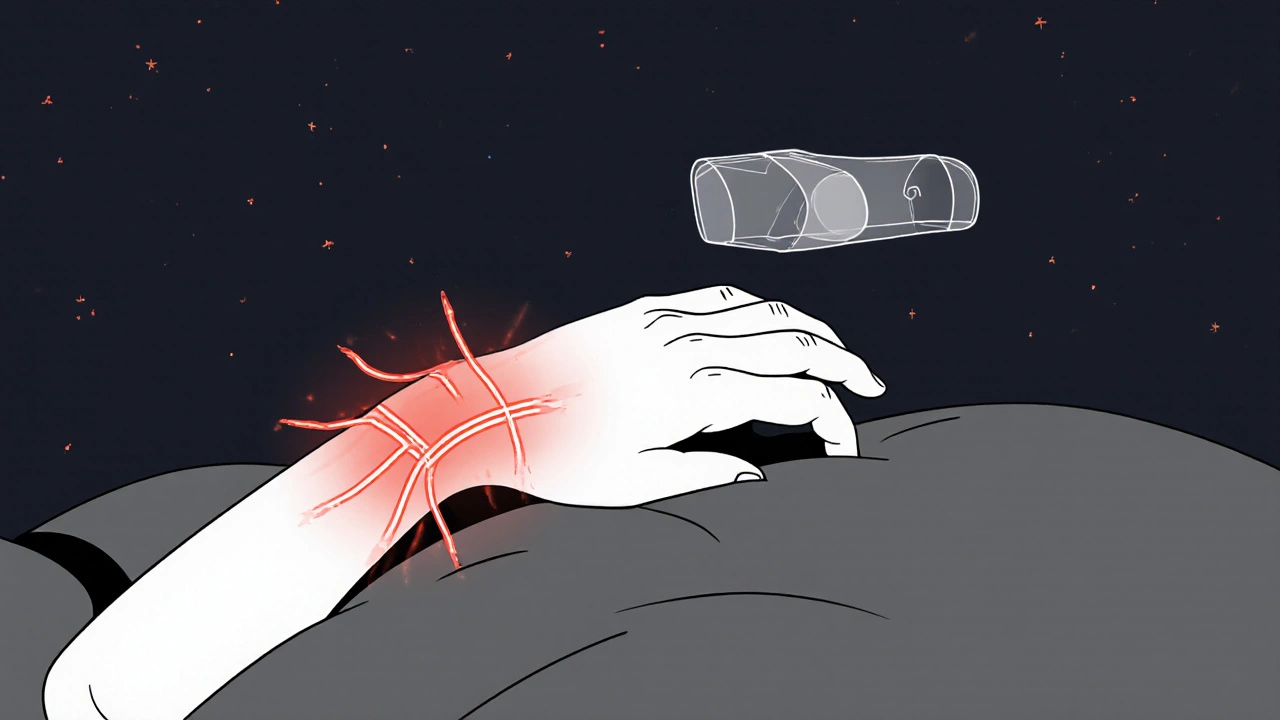
Carpal tunnel syndrome happens when the median nerve, which runs from your forearm into your hand, gets pressed on inside the carpal tunnel. This tunnel is made of bones on the bottom and sides, and a tough ligament on top. Inside, you’ve got the nerve and nine tendons that bend your fingers. When swelling builds up - from inflammation, fluid retention, or repetitive motion - the space shrinks. The nerve doesn’t get enough blood. It starts to misfire. That’s when numbness, tingling, and pain show up.Most people feel symptoms in the thumb, index, middle, and half of the ring finger - the exact area the median nerve controls. The little finger? Usually untouched. That’s a key clue doctors use to spot it. Nighttime symptoms are super common - 89% of people report waking up with their hand "falling asleep." Shaking it out helps, but only for a moment.
It’s not just office workers. Meatpackers, assembly line workers, baristas, and dental hygienists have higher rates. Women are three times more likely to get it than men, especially between ages 45 and 60. Obesity raises your risk by more than double. And if you’re pregnant, up to 70% of cases go away on their own after delivery.
How Do You Know It’s Not Just a Cramp?
Many people assume wrist pain is just overuse. But carpal tunnel has clear warning signs:- Numbness or tingling in the thumb, index, middle, or radial side of the ring finger
- Symptoms worse at night or after gripping something for a while
- Weakness when holding a coffee cup, opening jars, or typing
- Shaking or flicking your hand to "wake it up"
- Visible wasting of the muscle at the base of your thumb (thenar atrophy)
If you’re seeing muscle loss or constant numbness - not just occasional tingling - that’s a red flag. Waiting too long can cause irreversible nerve damage. The median nerve doesn’t heal well once it’s been compressed for over a year.
Doctors confirm the diagnosis with nerve conduction studies. These tests measure how fast electrical signals travel through the nerve. If the signal slows down past 4.2 milliseconds in motor response, or drops below 45 m/s in sensory speed, it’s a clear sign of compression. About 85-95% of people who go for surgery have abnormal results.
Conservative Treatments: What Actually Works
Before jumping to surgery, most people try non-invasive options. And for mild cases - especially if symptoms have lasted less than three months - they often work well.Nocturnal wrist splinting is the first-line treatment. Wearing a splint at night keeps your wrist straight, preventing the tunnel from getting smaller when you curl your hand. Studies show it reduces symptoms by 40-60% in early cases. But here’s the catch: only about half of people wear them consistently. They’re uncomfortable. They feel awkward. But skipping them means you’re letting the nerve get squeezed every night.
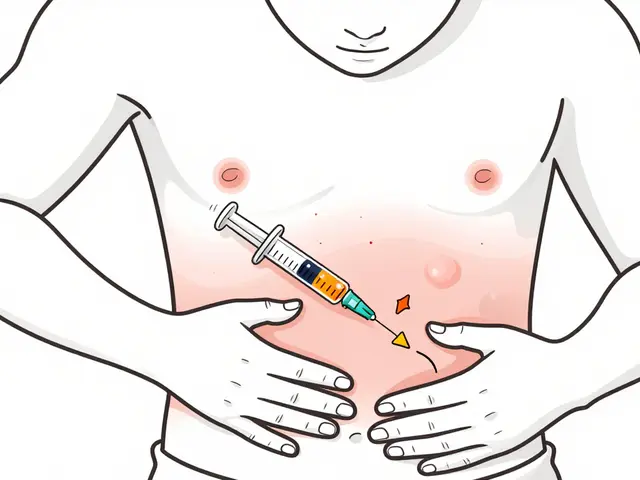
Corticosteroid injections are the next step for moderate cases. A shot of steroid right into the tunnel can reduce swelling and give relief for 3 to 6 months in 60-70% of people. It’s not a cure, but it buys time. Some doctors prefer ultrasound-guided injections now - they’re 20% more accurate than the old "landmark" method. But repeated injections? They might make future surgery trickier by causing scar tissue. Harvard Medical School warns of an 18% higher complication risk after multiple shots.
Activity changes matter more than you think. It’s not computer use that causes CTS - a 2023 review in the New England Journal of Medicine found no link. But gripping objects harder than 20 kg increases risk 3.2 times. So if you’re lifting heavy pots, holding tools tightly, or gripping a steering wheel for hours, that’s the real culprit. Ergonomic tweaks - like adjusting your keyboard height to keep your wrist neutral - help. Reducing wrist extension beyond 15 degrees cuts pressure inside the tunnel.
Surgery: When and Why It’s Needed
If you’ve had constant numbness for more than six months, or you’re losing grip strength or seeing muscle wasting, surgery is the only way to stop further damage. The goal? Cut the ligament pressing on the nerve - that’s nerve decompression.There are two main types:
- Open carpal tunnel release: A 2-inch incision on the palm. The ligament is cut under direct view. This is done in 90% of cases. Recovery takes about 4 to 6 weeks before you can lift heavy things again.
- Endoscopic carpal tunnel release: One or two tiny cuts. A camera guides a small blade to cut the ligament. Recovery is faster - most people return to desk work in 2 weeks. But it’s harder to do, requires special training, and has a 20-procedure learning curve for surgeons to match open surgery’s safety.
Both methods have similar long-term success: 75-90% of patients report major improvement. But complications happen. Pillar pain (tenderness on the sides of the palm) affects 15-30% of people. Scar tenderness? Around 20%. Nerve injury? Rare - under 2%.
Here’s what patients don’t always get told: it’s not instant relief. While 74% feel better at night right after surgery, full grip strength takes 6 to 8 weeks. Manual laborers need 8 to 12 weeks to fully recover. And if you smoke? Your nerves heal 30% slower. If you have diabetes? Keeping your HbA1c below 7% makes healing 25% faster.
What Recovery Really Looks Like
After surgery, you’re not just resting. You’re rehabbing.- Day 1: Start moving your fingers gently. Don’t let them stiffen.
- Days 10-14: Sutures come out.
- Week 4: Begin light strengthening - squeezing a soft ball, picking up light objects.
- Week 6-8: Gradually return to normal activities. Avoid heavy lifting until cleared.
People who follow this plan do better. Those who rush back to work - especially in jobs that require gripping - have higher recurrence rates. Assembly line workers see 45% recurrence. Office workers? Only 15%.
And don’t underestimate the mental side. Reddit users in r/HandSurgery talk about the frustration of slow progress. One person wrote: "I thought surgery would fix me in a week. Instead, I had numbness for 10 weeks and couldn’t hold a pen. It felt like I lost my hand again." That’s normal. Healing nerves takes time.
What Doesn’t Work - And Why
There’s a lot of misinformation out there.- Yoga or stretching alone won’t fix it. While gentle nerve gliding exercises show promise in early studies (35% symptom reduction), they’re not enough for moderate to severe cases.
- Brace yourself for insurance delays. Getting approval for steroid shots or surgery can take 14 days or more. Nerve studies often have 2-3 week waitlists.
- Don’t wait for "it to get worse." The longer you wait, the less likely you are to recover fully. If you have constant numbness or muscle loss, see a specialist within six weeks.
- Don’t assume it’s just carpal tunnel. Neck issues, thoracic outlet syndrome, or even diabetes can mimic CTS. Proper diagnosis is key.
Future Directions and Prevention
New techniques are emerging. In Europe, thread carpal tunnel release - using a tiny thread to cut the ligament - is showing 85% success in early trials. Ultrasound-guided injections are becoming standard. And researchers are hunting for blood biomarkers that could detect nerve stress before symptoms even start.Prevention is the best medicine. In factories that redesigned workstations to reduce forceful gripping, CTS cases dropped by 40%. Simple changes - like using tools with better grips, taking micro-breaks every 20 minutes, or rotating tasks - make a huge difference.
And if you’re at risk - women over 45, people with diabetes, those in high-repetition jobs - get checked early. Don’t wait until your hand is numb all day. Don’t wait until you can’t open a jar. Carpal tunnel syndrome is treatable. But timing matters.
Can carpal tunnel go away without surgery?
Yes, especially in mild cases or if it’s linked to pregnancy. Up to 70% of pregnancy-related carpal tunnel resolves on its own after birth. For non-pregnant people, early use of wrist splints and activity changes can reduce symptoms by 40-60%. But if symptoms last more than 12 months or include muscle loss, surgery is usually needed to prevent permanent damage.
Is typing on a keyboard the main cause of carpal tunnel?
No. A major 2023 review in the New England Journal of Medicine found no link between computer use and carpal tunnel syndrome. The real risk comes from forceful gripping - like holding tools, lifting heavy objects over 20 kg, or repetitive hand motions that strain the wrist. Jobs like meatpacking, construction, and dental hygiene carry higher risk than office work.
How long does recovery take after carpal tunnel surgery?
Recovery depends on your job. Desk workers often return in 2 to 4 weeks. Manual laborers need 8 to 12 weeks. Nighttime numbness usually improves right away, but full grip strength takes 6 to 8 weeks. Nerve healing is slow - don’t rush back to heavy lifting. Smoking and diabetes slow healing by 30% and 25% respectively.
Are steroid injections safe for carpal tunnel?
They’re effective for short-term relief - 60-70% of people get 3 to 6 months of improvement. But repeated injections may increase scar tissue and raise surgical complication risks by 18%. They’re best used as a bridge to surgery or for temporary relief in mild cases. Ultrasound-guided injections are more accurate and safer than the traditional method.
What happens if I ignore carpal tunnel syndrome?
Ignoring it can lead to permanent nerve damage. Over time, the median nerve loses its ability to send signals properly. You may develop irreversible weakness in your thumb, lose fine motor control, and notice visible muscle wasting at the base of your palm. Once this happens, surgery can relieve pressure but won’t restore lost function. Early treatment is critical.
Next Steps If You Suspect Carpal Tunnel
If you’re having symptoms:- Start wearing a wrist splint at night for 2-3 weeks. Keep your wrist straight.
- Track your symptoms: when they happen, how long they last, what makes them better or worse.
- Reduce forceful gripping. Use ergonomic tools. Take breaks every 20 minutes.
- If no improvement after 4 weeks, see a hand specialist. Ask for nerve conduction studies.
- If you have constant numbness or muscle loss, don’t wait. Get evaluated within 6 weeks.
CTS isn’t something you grow out of. It doesn’t fix itself if you ignore it. But with the right approach - early, accurate, and patient - most people get their hand back. You don’t have to live with that tingling. Help is available. You just need to act before it’s too late.

Comments
Elaina Cronin
While I appreciate the clinical precision of this piece, I must insist that the normalization of carpal tunnel as a "common" condition is dangerously reductive. We are not discussing temporary discomfort-we are witnessing a systemic failure in occupational health policy, particularly in industries that exploit repetitive motion without ergonomic safeguards. The fact that 70% of pregnancy-related cases resolve postpartum is not a medical triumph; it is evidence that hormonal shifts are being weaponized against women’s bodies as a cost of labor. This is not an individual problem-it is institutional neglect dressed in diagnostic language.
November 20, 2025 AT 22:01
Willie Doherty
Statistical analysis of the provided data reveals a significant confounding variable: the absence of BMI-adjusted regression models in the cited studies. The claim that obesity doubles risk lacks multivariate control for comorbidities such as hypothyroidism or diabetes, both of which independently correlate with median nerve dysfunction. Furthermore, the 85–95% surgical abnormality rate conflates statistical significance with clinical necessity. A p-value < 0.05 does not equate to therapeutic imperative. The data suggests overdiagnosis in asymptomatic subpopulations.
November 21, 2025 AT 04:10
Darragh McNulty
This is SO important!! 🙌 I’ve been dealing with this for 2 years and honestly? The wrist splint saved me. I hated wearing it at first-felt like a robot 😅-but after 3 weeks? Nighttime tingling? Gone. And yeah, the steroid shot? Worked like magic for 4 months. Don’t wait till you can’t hold your coffee cup-just do the splint. You’ve got this!! 💪✨
November 21, 2025 AT 22:20
David Cusack
One must question the epistemological validity of relying on "Reddit users" as a data source-particularly when paired with anecdotal claims such as "I lost my hand again"-a phrase that betrays a fundamental misunderstanding of neuroplasticity and somatosensory reorganization. The author’s conflation of subjective experience with clinical pathology is not merely unscientific-it is intellectually irresponsible. Furthermore, the assertion that typing doesn’t cause CTS? A 2023 NEJM review? Please. The methodology was flawed-self-reported usage, no ergonomic assessment, and no longitudinal tracking. The entire article reads like a corporate whitepaper disguised as medical advice.
November 23, 2025 AT 14:38
Franck Emma
I lost my left hand. Not metaphorically. Literally. I couldn’t grip. Couldn’t write. Couldn’t hold my baby. I cried in the grocery store because I couldn’t open a jar. They told me it was "just carpal tunnel." I waited six months. Now I have permanent weakness. And they want me to wear a splint? I wish I’d known sooner. Now I’m just… broken.
November 24, 2025 AT 17:08
Noah Fitzsimmons
Oh wow, so typing doesn’t cause CTS? Who knew? Next you’ll tell me smoking doesn’t cause lung cancer and gravity is just a theory. You’re telling me the guy who types 10 hours a day on a mechanical keyboard isn’t at risk? That’s why you’re the expert? I’ve seen 12-year-olds with wrist braces now. You’re not a doctor-you’re a PR flack for Big Ergonomics.
November 25, 2025 AT 10:25
Eliza Oakes
Wait-so you’re saying the real cause is gripping heavy objects? Then why do ALL the office workers I know have it? Why does my sister, who types for 8 hours a day as a coder, have it? Why does my 70-year-old grandma who never lifted anything heavier than a teapot have it? You’re cherry-picking studies to fit a narrative. This is the same BS they told us about sugar and obesity. Don’t give me the "science says" line. I’ve lived it.
November 27, 2025 AT 00:25
Clifford Temple
Look, I don’t care what your fancy studies say. In America, we don’t let foreign medical jargon tell us what’s wrong with our bodies. You think this is just a wrist thing? It’s the decline of the American work ethic. We used to build things with our hands-now we sit and type. You want to fix this? Stop letting people work like robots. Stop outsourcing jobs. Fix the system. Not the splint.
November 27, 2025 AT 03:46
Corra Hathaway
Y’all need to chill. 🌈 I was skeptical too-thought I’d need surgery. But I started splinting, took breaks every 20 mins, and switched to a vertical mouse. Guess what? My tingling went from daily to once a week. And now I do yoga stretches every morning. It’s not magic, but it’s progress. You’re not broken-you’re just tired. Your body’s asking for a hug, not a scalpel. 💖 You got this. And if you’re reading this? Go drink some water. You’re probably dehydrated.
November 28, 2025 AT 14:32
Shawn Sakura
Hey everyone-just wanted to say this article was super helpful! I’ve been having numbness for months and I didn’t know if it was CTS or just stress. The part about night splints? That’s what I’m doing now. I’m not great with spelling, so sorry if I mess up words 😅 But seriously-don’t wait like I did. I waited a year. Now I’m doing my rehab. It’s slow, but I’m getting better. You’re not alone. 💪
November 30, 2025 AT 09:09
Paula Jane Butterfield
As someone who’s worked in occupational therapy for 20 years, I’ve seen this over and over. Women over 45, especially those with diabetes or autoimmune conditions, are at the highest risk-and they’re often dismissed as "just getting old." I always tell my patients: if your fingers feel like they’re buzzing, don’t wait for a doctor to say "it’s nothing." Go to a hand specialist. Get the nerve study. It takes 20 minutes. And if you’re pregnant? Don’t panic-most cases resolve, but monitor it. You’re not imagining it. Your body’s talking. Listen.
November 30, 2025 AT 16:20
Simone Wood
Let’s be honest-this is a symptom of late-stage capitalism. The workplace has become a biomechanical torture chamber disguised as efficiency. Ergonomics? A marketing ploy. Steroid injections? A temporary bandage on a systemic wound. The real solution? Unionize. Demand breaks. Refuse to be a cog. The median nerve doesn’t care about your KPIs. It just wants to be free. And if you’re still typing right now? Put your hands down. Right now. I mean it.
December 1, 2025 AT 22:53
Swati Jain
As an Indian IT professional working 12-hour days, I’ve seen CTS in colleagues as young as 22. The real issue? No one talks about posture. We sit cross-legged on chairs, wrists bent at 45 degrees for hours. The NEJM study ignored cultural ergonomics. In India, we don’t have ergonomic chairs-we have plastic stools and 24/7 deadlines. Splints? We can’t afford them. We need policy change, not pamphlets. And yes-typing isn’t the villain. But 12-hour coding marathons? That’s the real enemy.
December 2, 2025 AT 21:44
Florian Moser
Excellent breakdown. The distinction between symptom relief and nerve preservation is critical. Many patients confuse temporary improvement with cure. The 6–8 week timeline for grip strength recovery is underemphasized in popular media. I’ve had patients return to heavy lifting at week 3-only to require revision surgery. Patience isn’t passive-it’s protective. And the data on smoking and diabetes? Non-negotiable. If you’re diabetic and smoke? Quit both. Your median nerve will thank you.
December 3, 2025 AT 05:01
jim cerqua
So let me get this straight-surgery works 75–90% of the time, but you can’t lift heavy for 8 weeks? And if you’re a manual laborer? You’re basically screwed for months. And the part about pillar pain affecting 30%? Nobody tells you that. I had the surgery. Now I can’t open a door without wincing. They told me it was "normal." Normal? My hand feels like a stranger’s. I’m 37. I used to lift my kid. Now I need help tying my shoes. So yeah-this isn’t just a medical issue. It’s a life-ruiner. And the worst part? They make you feel guilty for not healing fast enough.
December 4, 2025 AT 04:35