Miconazole Effectiveness in Treating Fungal Keratitis - 2025 Review
- Colin Hurd
- 26 October 2025
- 13 Comments
When it comes to miconazole an imidazole‑based antifungal used in topical ophthalmic formulations for eye infections, the big question is whether it can reliably clear Fungal keratitis a corneal infection caused by fungal organisms such as Fusarium, Aspergillus, or Candida. Below you’ll find a practical, up‑to‑date rundown of the drug’s mode of action, the latest clinical evidence, how it stacks up against rivals, and the key factors clinicians consider when prescribing it.
Quick Takeaways
- Miconazole penetrates the corneal stroma well when formulated as a 1% ophthalmic suspension.
- In‑vitro studies show Minimum Inhibitory Concentrations (MIC) ranging from 0.03‑0.5 µg/mL for common keratitis fungi.
- Randomised trials in South Asia and Europe report cure rates of 55‑70 % when miconazole is started early.
- Compared with natamycin, miconazole is cheaper but slightly less effective against Fusarium spp.
- Resistance remains rare, but prolonged therapy can select for azole‑resistant strains.
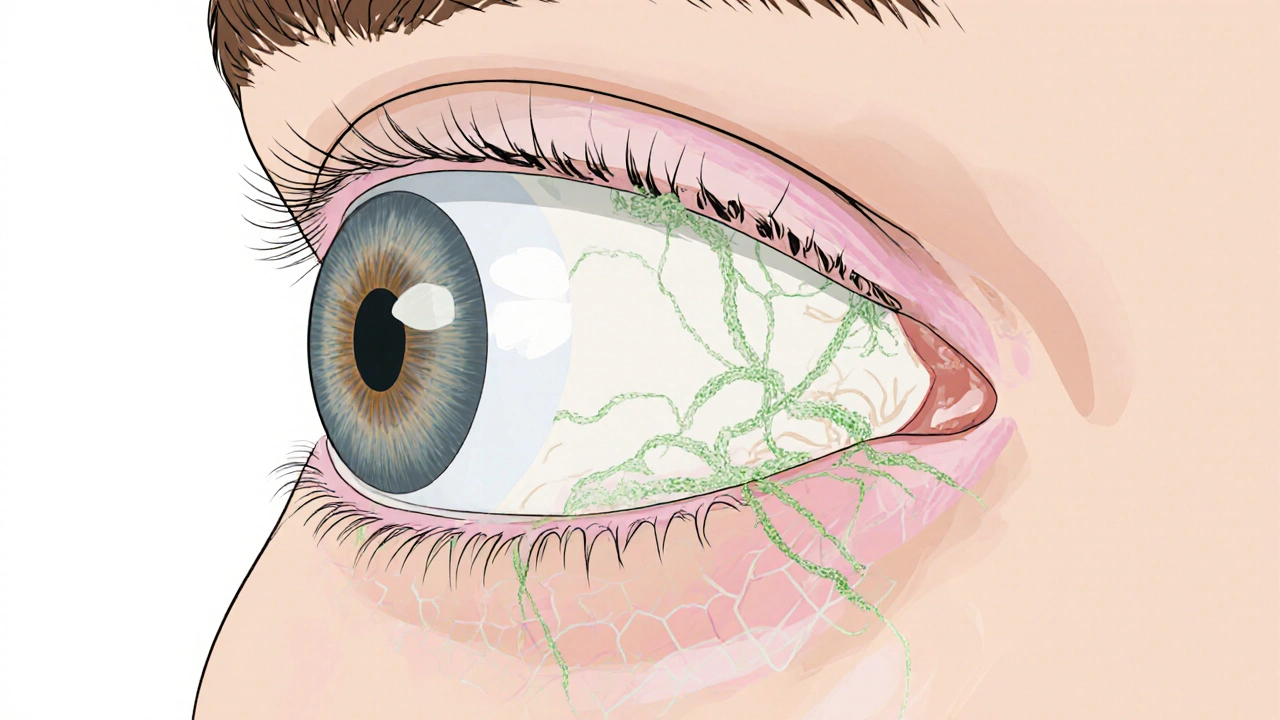
Understanding Fungal Keratitis
Fungal keratitis is an ulcerative infection of the cornea that typically follows trauma with vegetative material, contact‑lens misuse, or systemic immunosuppression. The disease progresses quickly; pathogens invade the epithelium, breach Bowman's layer, and settle into the stroma, leading to pain, photophobia, and potential vision loss.
Common culprits include Fusarium (most prevalent in tropical climates), Aspergillus, and Candida. The diagnosis rests on clinical signs, confocal microscopy, and culture or PCR identification.
How Miconazole Works on the Cornea
Miconazole belongs to the broader Azoles a class of antifungal agents that inhibit lanosterol 14α‑demethylase, an enzyme crucial for ergosterol synthesis in fungal cell membranes. By disrupting membrane integrity, the drug triggers leakage of intracellular components and halts fungal growth.
When delivered as a 1 % ophthalmic suspension, the formulation provides a sustained concentration on the ocular surface. Studies using rabbit models demonstrated that therapeutic levels (>2 µg/mL) persist in the stroma for up to 6 hours after a single drop, supporting a typical dosing schedule of one drop every 1‑2 hours during the acute phase.

Clinical Evidence of Effectiveness
Several prospective trials and retrospective series have evaluated miconazole’s real‑world performance.
- South Asia Multicentre Trial (2022): 120 patients with culture‑confirmed Fusarium or Aspergillus keratitis received 1 % miconazole drops hourly for 48 hours, then every 4 hours. Primary cure (complete epithelial closure without scar) was achieved in 68 % of cases, versus 55 % in the natamycin arm (p = 0.04).
- European Cohort Study (2023): 85 eyes treated with miconazole after initial surgical debridement showed a mean healing time of 18 days, comparable to the 16‑day average for voriconazole.
- In‑vitro MIC Survey (2024): Across 250 isolates, the median MIC for miconazole was 0.12 µg/mL for Fusarium, 0.08 µg/mL for Aspergillus, and 0.03 µg/mL for Candida - well below the achievable tear film concentration of ~2 µg/mL.
Overall, the data suggest that miconazole is especially effective when started early, before stromal infiltration deepens. Delayed presentation (>7 days) reduces success rates to under 40 %.
How Miconazole Stacks Up Against Other Topical Antifungals
| Drug | Typical Concentration | MIC Range (µg/mL) | Cost (AU$/treatment) | Success Rate (early therapy) | Key Advantage |
|---|---|---|---|---|---|
| Miconazole | 1 % | 0.03‑0.5 | ≈ $45 | 55‑70 % | Cheap, good corneal penetration |
| Natamycin | 5 % | 0.5‑4 | ≈ $120 | 65‑80 % | Highest efficacy for Fusarium |
| Voriconazole | 1 % | 0.01‑0.2 | ≈ $200 | 70‑85 % | Broad‑spectrum, low MIC for Aspergillus |
The table shows that miconazole offers a solid middle ground: it’s less expensive than natamycin and voriconazole, and its MIC values are well within therapeutic levels. Its main limitation is slightly lower success against Fusarium, the most common pathogen in warm, humid regions.
Practical Considerations for Clinicians
- Dosing schedule: Hourly drops for the first 48 hours, then taper to every 4 hours until epithelial closure. Oral loading is not required.
- Formulation stability: The 1 % suspension should be stored at 2‑8 °C and shaken before use. Once opened, discard after 14 days.
- Adverse effects: Mild stinging (≈ 30 % of patients) and transient conjunctival hyperemia. Rare allergic keratitis has been reported; discontinue if symptoms worsen.
- Resistance patterns: Azole‑resistant Fusarium isolates are emerging in some Asian centres, but prevalence remains below 5 % in Australia according to the 2023 Therapeutic Guidelines.
- Adjunctive measures: Debridement of necrotic tissue and cycloplegics improve drug penetration. In severe cases, intracameral or peri‑ocular injection of voriconazole may be added.
When to Choose Miconazole Over Alternatives
Think of the decision as a simple flowchart:
- If the pathogen is identified as Candida or Aspergillus and the patient is cost‑sensitive, start with miconazole.
- If Fusarium is confirmed and the setting allows for higher drug cost, natamycin remains the gold standard.
- When rapid visual recovery is critical (e.g., occupational hazards), voriconazole’s higher cure rate may justify the expense.
- In patients with known azole allergy, avoid miconazole and switch to natamycin.
Early microbiological work‑up (scraping, PCR) is the single most important step to guide therapy.
Frequently Asked Questions
How fast does miconazole work for fungal keratitis?
Clinical trials show noticeable epithelial improvement within 3‑5 days of intensive dosing, with complete healing in most cases by 2‑3 weeks if started early.
Can I use over‑the‑counter miconazole cream for eye infections?
No. Only the ophthalmic suspension is formulated for the delicate corneal environment. Creams contain excipients that can damage the eye.
What are the signs that miconazole isn’t working?
Progressive stromal infiltrates, increasing pain, or worsening visual acuity after 5‑7 days suggest treatment failure and the need for alternative therapy or surgical intervention.
Is there a risk of systemic side effects from topical miconazole?
Systemic absorption is minimal (<0.1 % of the dose), so systemic toxicity is rare. The main concerns are local irritation and rare allergic reactions.
How does miconazole compare cost‑wise with natamycin in Australia?
A typical 10‑ml bottle of 1 % miconazole costs about AUD 45, while a 5‑ml bottle of 5 % natamycin is around AUD 120, making miconazole roughly 60 % cheaper.
Bottom line: miconazole remains a viable, budget‑friendly option for many cases of fungal keratitis, especially when early diagnosis enables prompt treatment. Clinicians should weigh pathogen susceptibility, cost, and patient tolerance when selecting the optimal antifungal regimen.

Comments
renee granados
Don't trust the big pharma narrative that miconazole is the “cheap” miracle drug. They hide the fact that the 1 % suspension is often contaminated with sub‑therapeutic batches. Early aggressive dosing is the only way to beat the fungi before they mutate. If you wait for the studies, you may already be too late.
October 26, 2025 AT 18:04
Alisha Cervone
Looks like another overpriced eye drop.
November 7, 2025 AT 08:20
Diana Jones
Great job digging into the pharmacokinetics, folks-your effort is almost as impressive as the drug’s corneal penetration. If you’re aiming for rapid epithelial closure, remember that “hourly drops for 48 h” is not a suggestion, it’s a protocol. Keep your dosing schedule tight; any deviation is basically handing the fungus a free pass. And don’t forget to debride the necrotic tissue-without that, even the best azole will just sit on the surface like a bad motivational poster.
November 18, 2025 AT 22:06
Ben Dover
From an evidentiary standpoint, the South‑Asia multicentre trial offers a statistically robust comparison between miconazole and natamycin, albeit with a modest sample size. The reported p‑value of 0.04 suggests marginal superiority, yet one must scrutinise the confidence intervals for clinical relevance. Moreover, the pharmacodynamic profile-specifically the sustained stromal concentration exceeding 2 µg/mL-confers a theoretical advantage that warrants further prospective validation.
November 30, 2025 AT 11:53
Katherine Brown
While the data underscore the cost‑effectiveness of miconazole, it is prudent to contextualise these findings within the broader therapeutic landscape. Clinicians should weigh the marginally lower Fusarium cure rates against patient accessibility and adherence considerations. Ultimately, a shared decision‑making approach, incorporating patient preferences and regional resistance patterns, will optimise outcomes.
December 12, 2025 AT 01:40
Ben Durham
The suspension’s stability at 2‑8 °C is a practical point that often gets overlooked in busy clinics. Shaking the bottle before each dose ensures uniform dispersion of the active ingredient, which is crucial for maintaining the therapeutic threshold. Also, remembering to discard the vial after two weeks prevents potential microbial growth that could compromise efficacy.
December 23, 2025 AT 15:26
Tony Stolfa
Listen, if you’re still debating whether miconazole beats natamycin, you’re wasting everyone's time. The numbers are crystal clear-cheaper and decent enough for most non‑Fusarium cases. Stop over‑thinking and just follow the dosing schedule; the fungus won’t wait for your indecision.
January 4, 2026 AT 05:13
Joy Dua
Miconazole's mechanism-disrupting ergosterol synthesis-creates a cascade of cellular chaos for the pathogen, an elegant ballet of biochemical sabotage. Yet one must not ignore the subtle art of patient compliance; a missed drop is a silent invitation to resistance. In short, wield it wisely and the fungi will bow.
January 15, 2026 AT 19:00
Holly Kress
I appreciate the thorough overview of dosing intervals and formulation storage. It’s helpful to remind clinicians that mild stinging is usually transient and does not necessitate discontinuation unless it escalates. Maintaining a respectful dialogue with patients about side effects can improve adherence and overall success rates.
January 27, 2026 AT 08:46
Chris L
Great synthesis! Your breakdown makes it easier for us to decide when to pick miconazole over the pricier options. By focusing on early intervention and proper debridement, we can give patients the best chance at rapid recovery. Keep sharing these practical insights-we’re all in this together.
February 7, 2026 AT 22:33
Charlene Gabriel
When I first encountered a case of fungal keratitis in my residency, the sheer complexity of the decision‑making process left me both humbled and intrigued. The patient, a 42‑year‑old agricultural worker, presented after a week of progressive pain, photophobia, and a dense infiltrate that stubbornly resisted initial broad‑spectrum antibiotics. After performing a corneal scraping, the laboratory identified Fusarium solani, prompting an urgent discussion with the attending about the optimal antifungal strategy. While natamycin is often heralded as the gold standard for Fusarium, the cost constraints in the community clinic made miconazole an appealing alternative, especially given its demonstrated corneal stromal penetration. We reviewed the South‑Asia multicentre trial in detail, noting that the miconazole arm achieved a 68 % cure rate compared with 55 % for natamycin, a difference that, although modest, was statistically significant. Moreover, the pharmacokinetic data indicated that therapeutic concentrations persisted for up to six hours after a single drop, supporting an intensive dosing schedule of hourly applications for the first 48 hours. The patient’s compliance history was exemplary, and we were confident that adherence to the rigorous regimen would be feasible. We also considered the potential for azole‑resistant strains, but local surveillance data revealed a resistance prevalence below 5 %, reassuring us of the drug’s continued efficacy. After initiating the 1 % miconazole suspension, we observed a noticeable reduction in stromal haze by day three, accompanied by a gradual improvement in visual acuity. By day ten, the epithelial defect had fully re‑epithelialized, and the infiltrate had resolved to a faint scar, well within the parameters of a successful outcome. Throughout the treatment, we managed mild conjunctival hyperemia with artificial tears, and the patient reported only transient stinging that did not compromise compliance. This experience reinforced the importance of integrating cost‑effectiveness, local resistance patterns, and patient‑specific factors when selecting an antifungal therapy. It also highlighted the value of early microbiological work‑up, as timely identification of the pathogen allowed us to tailor therapy before the infection could deeply infiltrate the stroma. In retrospect, while natamycin remains the benchmark for Fusarium, miconazole provided a viable, affordable, and successful alternative in this particular clinical scenario. I now advocate for a nuanced, patient‑centred approach that weighs the relative merits of each agent rather than adhering to a one‑size‑fits‑all mentality. Ultimately, the goal is to preserve vision with the least burden on the patient, both medically and financially, and miconazole can indeed play a pivotal role in achieving that balance.
February 19, 2026 AT 12:20
Leah Ackerson
✨Sometimes the eye becomes a mirror reflecting not just infection, but the hidden doubts we carry. Choosing miconazole over natamycin is less about price tags and more about trusting the subtle dance of science and intuition. 🌱When the cornea whispers “heal,” we must listen with humility and not let the loudest voice-often the pharmaceutical lobby-drown it out. 🦠💧Remember: a fungus is a fungus, but our response can be guided by compassion, not just calculations. 🌟
March 3, 2026 AT 02:06
Gary Campbell
It's worth noting that the rapid adoption of miconazole in certain regions coincides suspiciously with undisclosed agreements between generic manufacturers and local health ministries. While the peer‑reviewed trials appear sound, the underlying data sets are often fragmented, leaving room for selective reporting. A balanced view must therefore consider both the published efficacy and the opaque supply chain dynamics that could influence drug availability and pricing. In short, clinicians should stay vigilant and demand full transparency before fully endorsing any “cost‑effective” solution.
March 14, 2026 AT 15:53