Insulin Injection Site Reactions: How Lipodystrophy and Bruising Affect Blood Sugar Control
- Colin Hurd
- 24 March 2026
- 9 Comments
Lipodystrophy Risk Assessment Tool
This tool helps you assess your risk of developing lipodystrophy from insulin injections. Answer the questions below to determine your risk level and receive personalized recommendations.
1. Do you experience lumps, dents, or bruises at your injection sites?
2. How do you rotate injection sites?
3. Do you reuse insulin needles?
4. Do you notice bruising after injecting?
5. How often do you check your injection sites?
When you inject insulin every day, it’s easy to think the only thing that matters is getting the dose right. But what happens where the needle goes? If you’ve noticed lumps, dents, or bruises at your injection spots, you’re not alone-and these aren’t just skin-deep issues. They directly mess with your blood sugar control, sometimes in dangerous ways.
What Exactly Is Lipodystrophy?
Lipodystrophy isn’t one thing-it’s two opposite problems that both happen because of repeated insulin injections in the same spots. The most common form is lipohypertrophy: fat builds up under the skin, creating soft, rubbery lumps that can be as big as a golf ball. These lumps usually show up on the abdomen, thighs, or arms-where most people inject. The second form is lipoatrophy: fat disappears, leaving shallow dents or indentations in the skin. Both are caused by how your body reacts to insulin over time, not by infection or poor hygiene.Studies show lipohypertrophy affects between 30% and 50% of people using insulin long-term. In people with type 1 diabetes, that number can climb to 50%. It’s not rare. It’s common. And it’s often missed. Many patients don’t realize the lump they’ve been injecting into for months is actually a problem. Why? Because those areas often feel numb. So you don’t feel pain. You think it’s safer. But it’s the opposite.
Why Do These Lumps and Dents Form?
It starts with rotation-or the lack of it. If you keep injecting in the same small patch of skin, your body responds by building extra fat (lipohypertrophy) or breaking down fat (lipoatrophy). The exact reason isn’t fully understood, but insulin itself seems to trigger inflammation and tissue changes. Long-acting insulins like Lantus or Levemir are more likely to cause this than short-acting ones, simply because they stay in the tissue longer.Needle reuse makes it worse. Using the same needle over and over dulls the tip, which tears tissue instead of sliding in cleanly. That trauma adds to the buildup of scar tissue and fat. A 2023 study found that 901 out of 1,370 insulin users had visible bruising-nearly 66%. Most of those cases were linked to pressing too hard on the injection pen or reusing needles.
Microscopically, the fat cells in lipohypertrophic areas are about twice the size of normal ones. They cluster together, forming dense, uneven pockets. That’s why insulin injected there doesn’t absorb properly. Instead of going in smoothly, it’s delayed, uneven, and unpredictable. That’s why people with unexplained high blood sugar one day and sudden lows the next often have hidden lipohypertrophy.
How Bruising Fits In
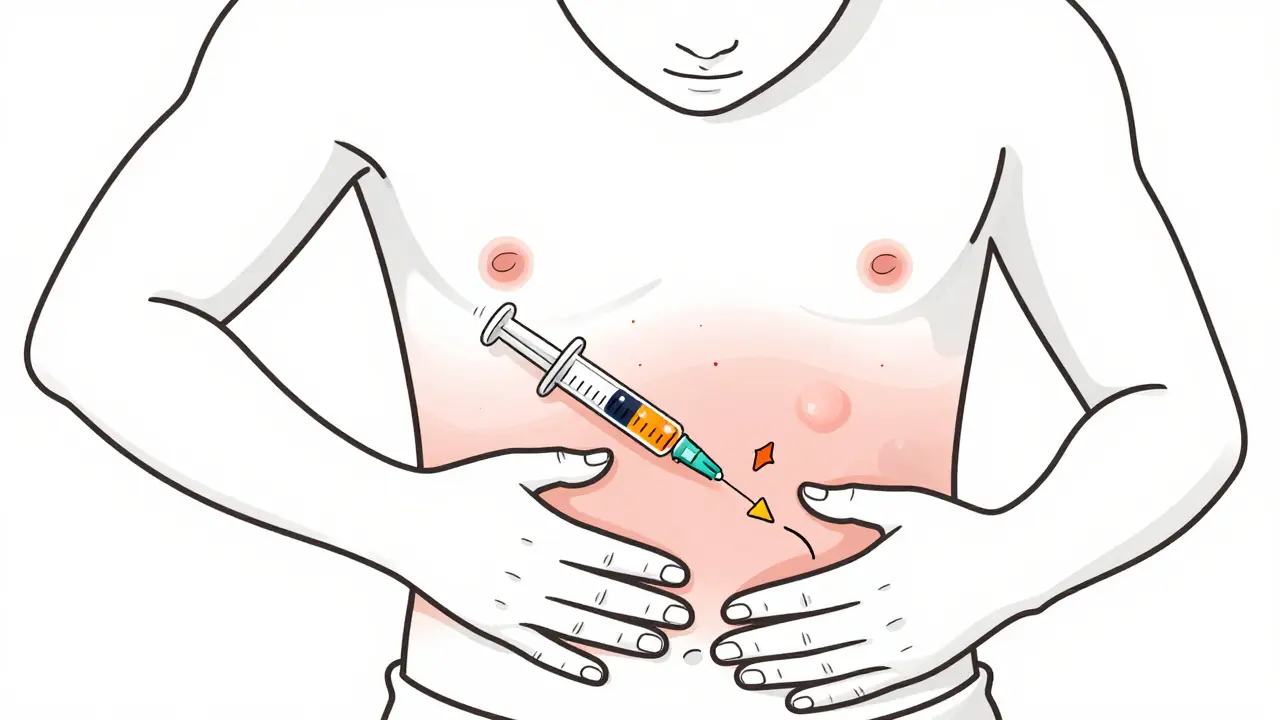
Bruising isn’t the same as lipodystrophy, but it’s a red flag. If you’re seeing purple or yellow marks after injecting, it usually means you hit a small blood vessel or are pressing too hard. Unlike lipohypertrophy, bruising goes away in a few days. But if it keeps happening in the same spot, it’s a sign you’re not rotating well-or you’re using the wrong needle.Most people who bruise often use needles that are too thin (like 31G) or inject too quickly without stabilizing the skin. A simple fix? Pinch the skin before injecting, especially if you’re thin. And after the shot, hold pressure for 5-10 seconds-don’t rub. Rubbing breaks more capillaries. Gentle pressure stops the bleeding.
One user on a diabetes forum said, “I used to bruise every time I injected. After switching to 32G needles and holding pressure, my bruises dropped by 80% in two weeks.” That’s not magic. That’s physics.
The Real Danger: Blood Sugar Chaos
The biggest problem with lipodystrophy isn’t how it looks. It’s how it messes with your insulin absorption. When you inject into a lump, your body absorbs the insulin slowly and unevenly. That means:- Your blood sugar spikes because insulin doesn’t work when you expect it to
- You get unexplained lows because insulin suddenly kicks in hours later
- You end up taking more insulin to compensate, which makes the lumps grow bigger
Research shows people with undiagnosed lipohypertrophy have 3.2 times more unexplained hypoglycemia and 2.7 times higher risk of diabetic ketoacidosis (DKA). One study found that patients with lipodystrophy needed 20-30% more insulin just to reach the same blood sugar levels as someone injecting into healthy tissue. That’s not a coincidence. That’s a direct result of poor absorption.
And here’s the cruel twist: people with lumps often prefer injecting into them because they’re numb. Less pain = more comfort. But that comfort is slowly destroying your glucose control.
How to Spot Lipodystrophy
You can’t always see it. That’s why palpation matters. Run your fingers over your injection areas every week. Look for:- Raised areas larger than 1 inch (2.5 cm)
- Firm, rubbery, or bumpy patches
- Areas that feel different from the surrounding skin
- Shallow dents or depressions
Don’t rely on sight. Many lumps are hidden under fat. Use your hands. If you feel something odd, avoid injecting there for at least 4-8 weeks. Let the tissue heal. And if you’re unsure, ask your diabetes educator to check your sites during your next appointment. Most don’t.
A 2023 survey found that 61% of insulin users said their doctor never checked their injection sites in five years. That’s unacceptable. Your injection sites are just as important as your A1c.
How to Prevent and Fix It
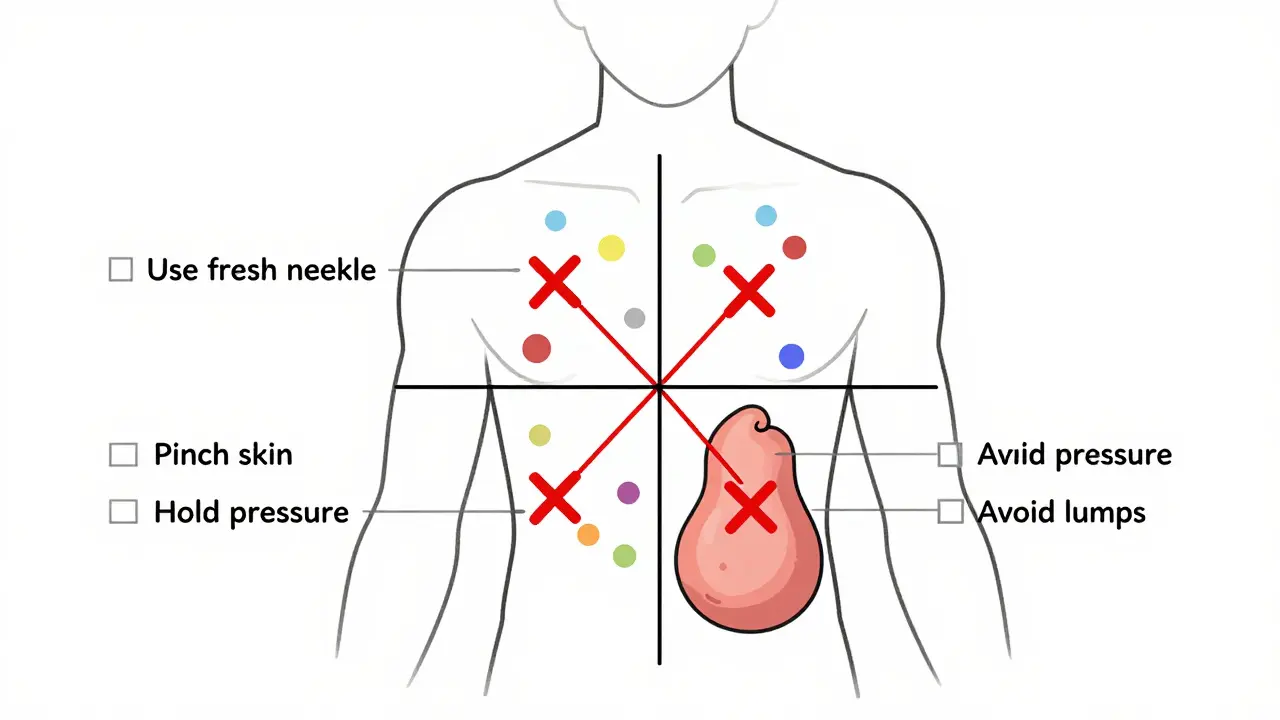
The solution is simple. But it takes discipline.- Rotate systematically. Divide your abdomen into four quadrants. Use one quadrant per week. Move at least 1 inch (2.5 cm) between each injection. Don’t just circle the same spot.
- Use fresh needles. Never reuse. A single needle should be used once. Dull needles cause more trauma, more bruising, and more tissue damage.
- Don’t inject into lumps. Even if they’re numb. Mark them with a pen or take a photo. Avoid them completely until they flatten out-sometimes that takes months.
- Pinch the skin. Especially if you’re lean. It lifts fat away from muscle, reducing the chance of hitting a vein.
- Hold pressure after injection. For 5-10 seconds. No rubbing. Just gentle, steady pressure.
Structured education reduces lipohypertrophy by 47%. That means if you learn the right technique, your risk drops sharply. YouTube channels like “All About Diabetes” have step-by-step rotation demos with 92% viewer-reported improvement. Apps like InPen track your injection sites and remind you where not to inject next. These tools aren’t fancy-they’re necessary.
What’s Changing Now
The industry is waking up. In 2023, Glooko released an AI tool that maps your injection sites and flags overused areas. In a 6-month trial with 450 users, it cut lipohypertrophy by 31%. Abbott announced a new glucose-responsive sensor for 2025 that will monitor tissue health at injection sites in real time. These aren’t sci-fi-they’re coming soon.But the biggest barrier isn’t technology. It’s awareness. Most patients don’t know this is a problem. Most providers don’t check for it. That’s changing slowly. The International Injection Technique Group now operates in 37 countries, training clinicians to look for these signs.
Bottom Line
Lipodystrophy and bruising aren’t cosmetic issues. They’re metabolic ones. Every time you inject into the same spot, you’re risking unstable blood sugar, unpredictable lows, and higher insulin needs. The fix isn’t new drugs. It’s better habits. Rotate. Don’t reuse. Check your skin. Stop ignoring the lumps.If you’ve been injecting for years and your A1c keeps creeping up despite no changes in diet or insulin dose-look at your skin. The answer might be right under your fingers.
Can lipohypertrophy go away on its own?
Yes, but it takes time-usually 2 to 6 months. The key is stopping all injections in that area. Once you avoid it completely, the body slowly breaks down the excess fat and scar tissue. If you keep injecting into the lump, it will only get worse. Some people see improvement in 8 weeks; others need 6 months. Patience and discipline are essential.
Is lipoatrophy still common today?
Much less common than lipohypertrophy. Lipoatrophy was more frequent in the 1980s and 1990s with older insulin formulations that triggered strong immune reactions. Modern insulins are highly purified and almost never cause lipoatrophy. If you see a dent, it’s more likely due to fat loss from poor circulation, weight loss, or long-term pressure on the area-not an allergic reaction.
Why do I bruise more on my thighs than my stomach?
Thigh skin is thinner and has more blood vessels close to the surface. The abdomen has thicker fat layers, which cushion the needle. If you’re bruising more on your thighs, try pinching the skin before injecting and use a slightly longer needle (like 8mm instead of 5mm) to ensure the insulin goes deep enough. Also, avoid injecting right after exercising-the blood flow increases, making veins more prone to puncture.
Can I inject into a bruised area?
No. Wait until the bruise is completely gone-usually 5 to 7 days. Injecting into a bruised area can cause more bleeding, increase pain, and interfere with insulin absorption. Even if the skin looks healed, the tissue underneath is still recovering. Always choose fresh, unbruised skin.
Do I need to change my insulin if I have lipodystrophy?
Not necessarily. The issue isn’t the insulin type-it’s where you’re injecting. Switching to a different insulin won’t fix a lump. The fix is changing your injection technique: rotate properly, avoid lumps, use fresh needles. However, if you’re on a long-acting insulin and keep developing lumps, your doctor might consider switching you to a shorter-acting one, as they’re less likely to cause tissue buildup.



Comments
Korn Deno
It's not about the needle or the insulin. It's about the system that lets us keep doing the same thing over and over without checking if it's still working. We treat diabetes like a math problem when it's actually a living, breathing mess of biology and habit. The body remembers. It holds onto trauma. And we keep ignoring it because it's easier than changing our routine.
Rotating sites isn't a tip. It's a ritual of respect.
March 26, 2026 AT 02:04
Natasha Rodríguez Lara
I used to inject in the same spot on my thigh for years because it was numb. Then one day I got a random low at 3 AM and nearly passed out. Turned out the lump was the size of a lemon. My endo didn't even check until I asked. Now I feel around every Sunday with my fingers. It's weird but it saves my life. Also, pinching the skin works. Try it.
March 27, 2026 AT 12:55
Kevin Siewe
This is one of those things that gets overlooked because it's not glamorous. No one posts about lumps on Instagram. But if you're struggling with unexplained highs and lows, this is the first thing to check. I teach this to every new patient I work with. Simple fix. Huge impact. Don't wait for a crisis.
March 27, 2026 AT 17:39
Chris Farley
So let me get this straight. We're blaming insulin for causing fat buildup? What's next? Are carbs making us fat now too? This whole thing feels like Big Pharma's way of selling you new pens and needles. You're injecting into a lump because it's numb? Good. That means it's working. Stop listening to these overeducated bloggers.
March 29, 2026 AT 06:23
Darlene Gomez
I love how this post doesn't just dump facts. It shows the human side. The numbness. The comfort. The shame. I used to hide my lumps under baggy pants. Thought I was the only one. Turns out half of us have them. And nobody talks about it. I started taking photos of my injection sites every week. It helped me see the pattern. I'm not fixed. But I'm trying. And that's enough for now.
March 30, 2026 AT 13:11
Katie Putbrese
You people are so naive. The government and the pharmaceutical companies want you to believe this is about technique. But it's not. They profit from you injecting into lumps because you need more insulin. More visits. More sensors. More drugs. This whole rotation thing? A distraction. The real solution is getting off insulin entirely. But they'll never tell you that.
March 31, 2026 AT 21:00
Donna Fogelsong
They're monitoring your injection sites with AI because they're building a database. Every time you inject, they're tracking your body's response. This isn't about health. It's about predictive modeling for insurance denial. You think they care if your A1c is high? No. They care if your data looks like a risk. Stop using those apps. Use paper. Write it down. Burn it.
April 1, 2026 AT 11:43
Sean Bechtelheimer
I tried pinching my skin and holding pressure... it worked 😊
April 2, 2026 AT 06:56
rebecca klady
I just started doing this last month. I was injecting into my old lumps out of habit. Now I mark them with a pen. Took me two weeks to stop. But my numbers are finally stable. No magic. Just paying attention.
April 3, 2026 AT 01:56